It’s rare that I am left speechless for long, but last Thursday was such an occasion. It has taken me until today to be able to put into words what happened and why it’s unjust and devastating. I gave myself a few days to breathe, to process, to regroup before attempting to write about it here.
I have spent the past eight years learning as much as I can about Newborn Screening from all possible angles and perspectives to prepare for the addition of Krabbe Disease to the RUSP, and as of Thursday, all of our plans and strategies came to a screeching halt (a temporary halt, but one nonetheless).
(this will be long but it’s mainly for my own future reference)
As a quick background for context, in order for a condition to be included on the federal Recommended Uniform Screening Panel (RUSP) it must undergo a rigorous review by the Advisory Committee on Heritable Disorders in Newborns and Children (ACHDNC) which is part of the Department of Health and Human Services. It’s a lengthy process (nine months once they decide to accept the condition for review) and the nomination packages are hundreds of pages thick, filled with data from experts, etc.
Last July, Hunter’s Hope Foundation submitted the nomination package for Krabbe Disease to be added to the RUSP. We were all so excited! While I wasn’t part of that process, my work in Pennsylvania has continued to provide much-needed data to support the nomination and I am so grateful for that. We were accepted into “Full Evidence Review” and Krabbe has been the main topic of discussion for the past three meetings.
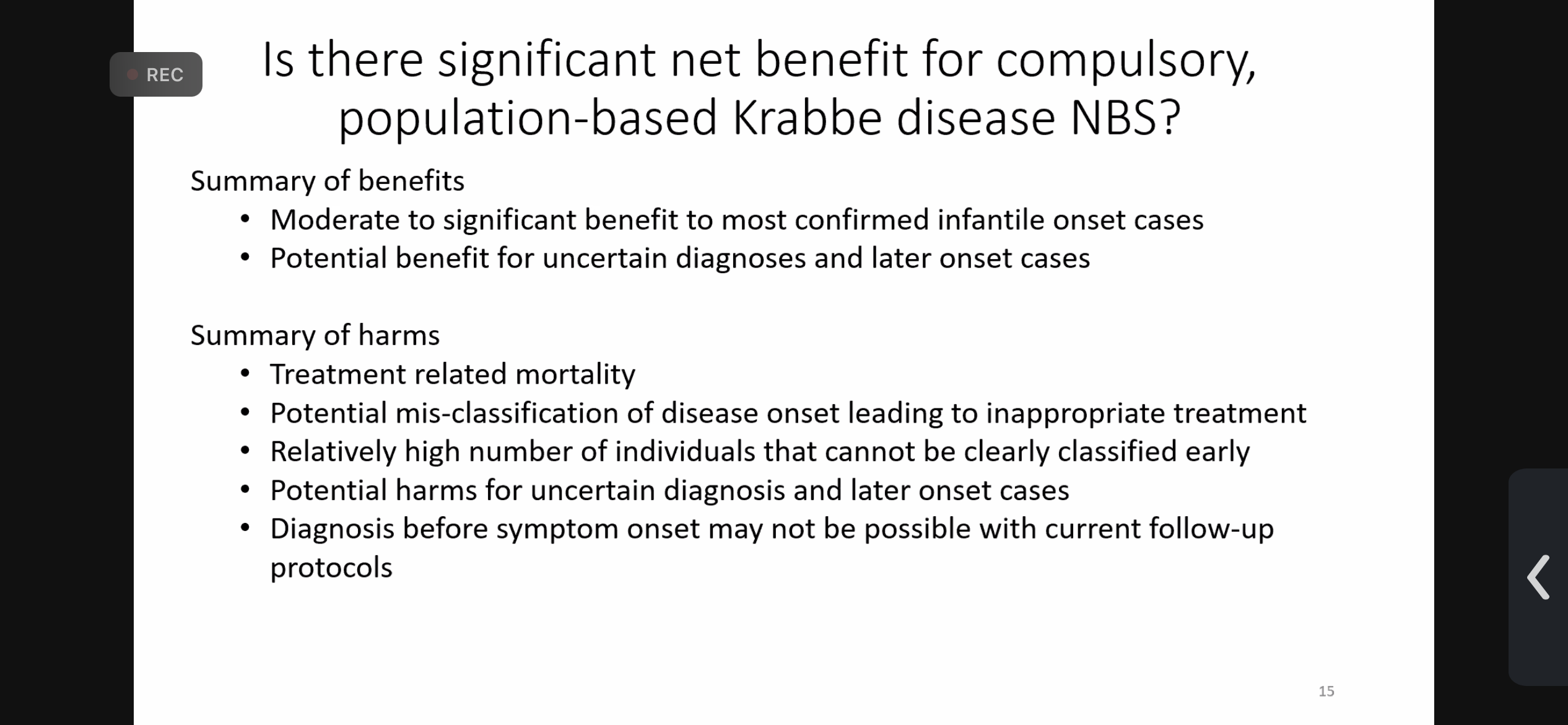
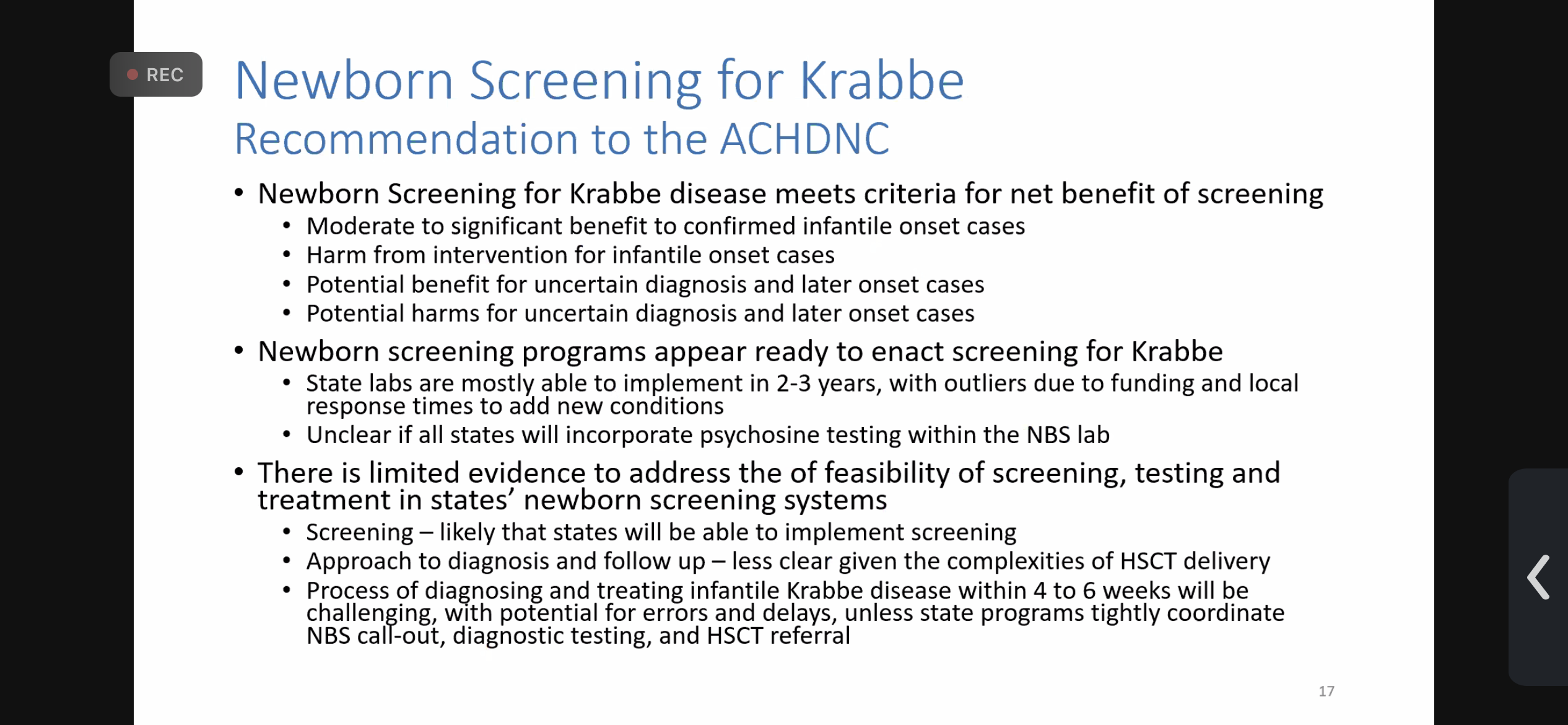
Our “day in court” arrived last week via the virtual meeting and as I listened to the discussion in the morning I felt optimistic. Dr. Kemper was presenting the evidence fairly well and it seemed positive. All of this changed after lunch when the conversation switched to a “Risk/Benefit” discussion and the rest felt like a bad dream.
Here are some of my screenshots:
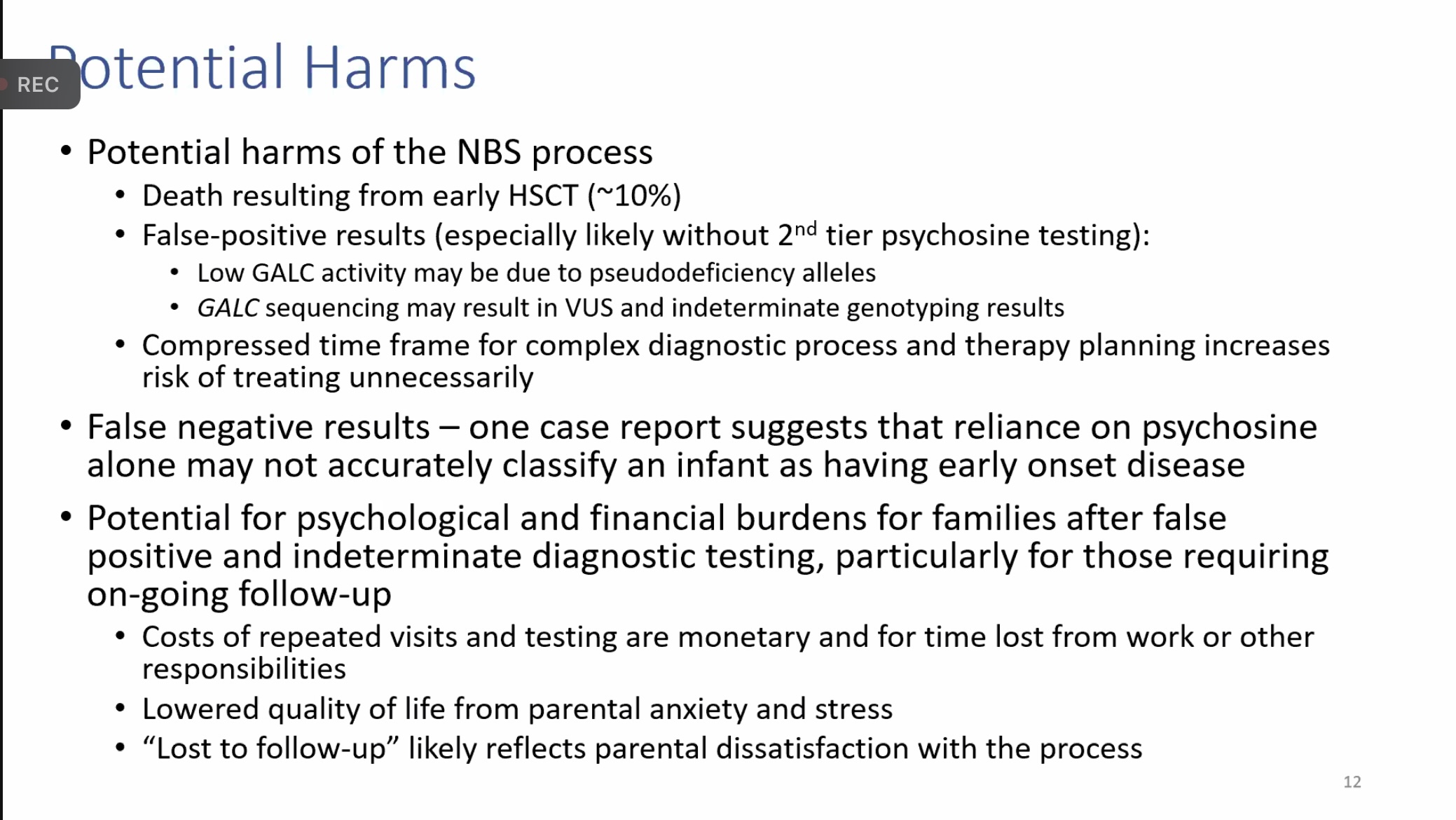
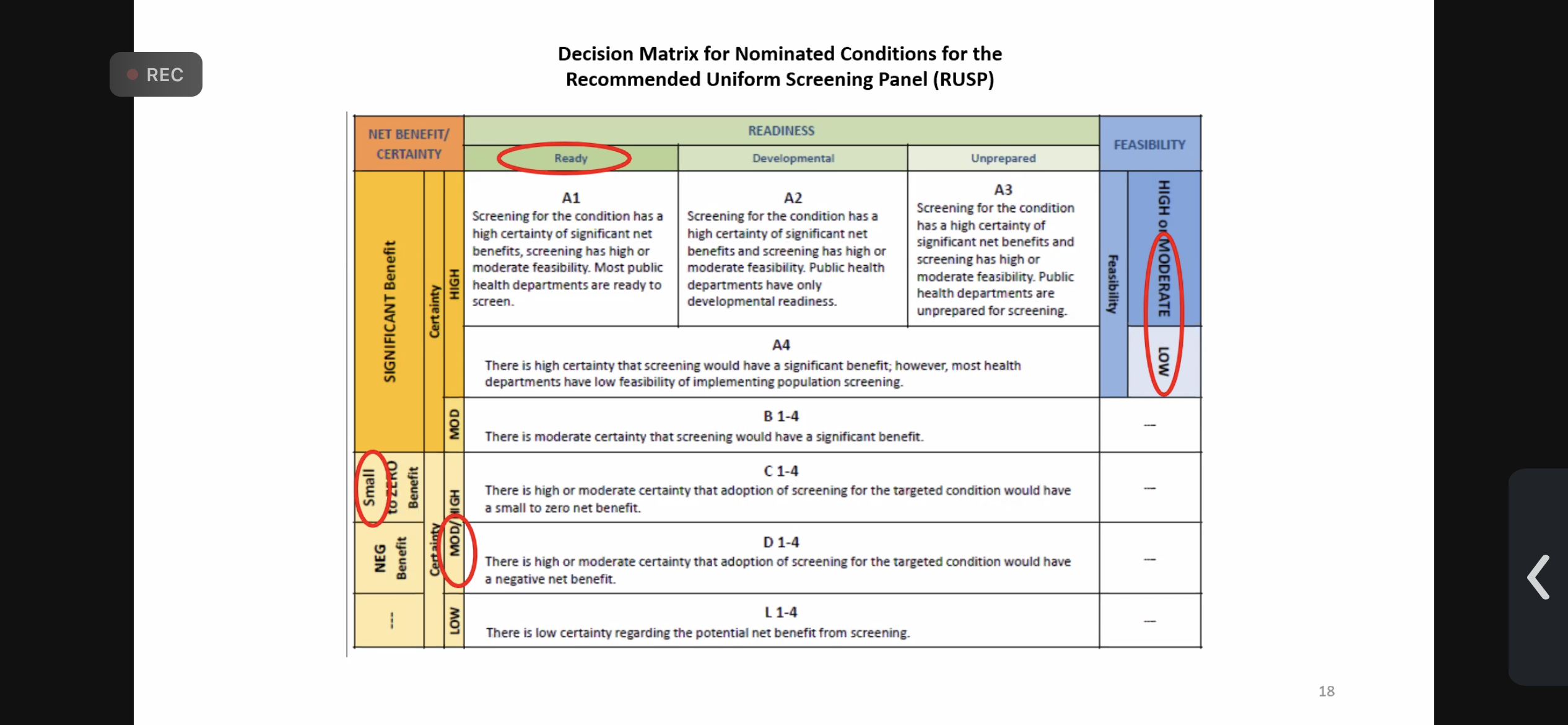
As I kept myself busy by cleaning the house and doing laundry, I listened to them discuss Krabbe in a completely different tone and I knew we were in trouble. They used inaccurate and outdated data, completely left out (and misrepresented) the parental perspective, and more.
One memorable point of discussion was regarding the 10% chance of death as a result of a stem-cell transplant (which is also inaccurate – it’s 5% or less) and they decided that was too risky. I actually yelled at my phone at that point because the alternative to not treating the child is a 100% chance of death.
Parents aren’t looking for perfection (in treatment) –
Lesa Brackbill
they are longing for options.
And for Krabbe Disease, those options are only presented
when a child is diagnosed EARLY.
As Dr. Escolar said yesterday, “You must have the parent voice in the conversation because you’re not the one living the risk.” In fact, many of the comments made were quite ableist in nature and I was shocked.
Another frustrating comment made was regarding patient outcomes when there is a family history (i.e. when a child has already had the disease and/or died) versus Newborn Screening and the assertion was made that the outcomes are better (which isn’t backed up by data). What I took from that part of the discussion was that they were actually considering whether or not it was better for the family to lose a child in order to save another rather than recommend that all states screen for Krabbe. Whether that’s what they meant or not is uncertain, but it was noted.
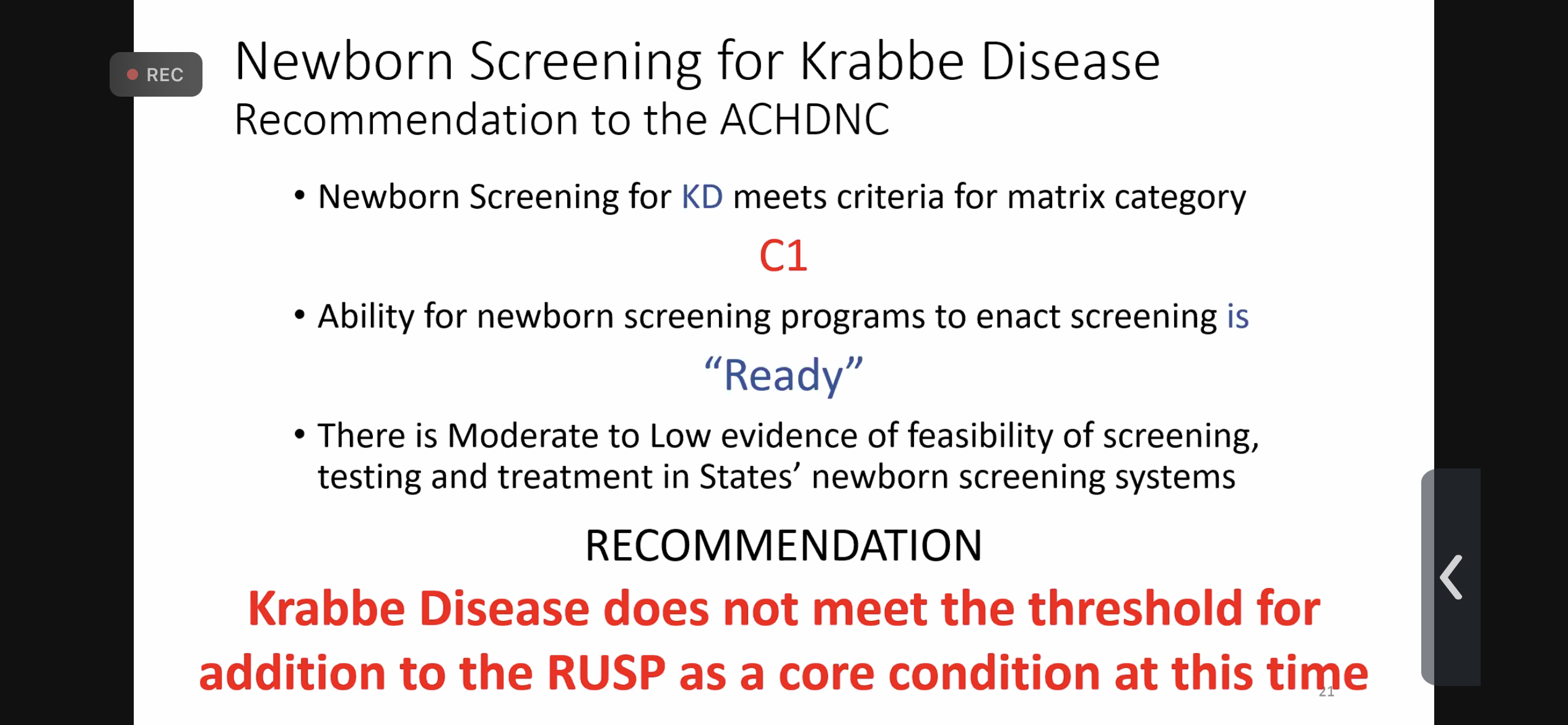
In the end, they decided that the benefit didn’t outweigh the risk (!!!) and they voted 7-7 (a tie, which should not be allowed based on their own statute) to not recommend Krabbe Disease to the RUSP.
This is where I’m grateful that so many in the Rare Disease community were watching and making observations while we cried because they noticed things I didn’t immediately see.
This is what Annie Kennedy from the EveryLife Foundation posted on LinkedIn that evening after she called me:
Completely dumbfounded.
I have been a part of the #newbornscreening community for more than 2 decades. Today, I listened to the #evidencereview for the nomination of #Krabbedisease to the #RUSP and heard the #Krabbe patient community provide impactful #patientexperience data before the Advisory Committee for Heritable Disorders for Newborns and Children. The Krabbe community’s engagement has included life saving newborn screening programs in 10 states, a life saving therapeutic intervention, and organized provider and patient community outreach efforts. Testimony today came from families who’d lost children, as well as those who’d both lost children and those whose children had been saved through stem cell transplant because of early detection. And heart wrenching testimony from parents of both. And a powerful testimony from a 12 year old young man with Krabbe who received transplant and lives a healthy life – all because of the diagnosis of an older sibling who had not benefited from treatment as early. THIS is why early detection and intervention is necessary.
But somehow… mind blowingly… after decades of effort and hundreds of childrens’ lives lost – today’s vote yielded a tie. Krabbe will NOT being moving forward for addition to the RUSP.
How is this possible?!
I am dumbfounded that Krabbe is not moving forward for addition to the federal panel today.
If – after pilots and data collection and construction of infrastructure and meaningful collaboration with stakeholders – we cannot ensure that every baby born in this country will have access to state-of-the-art screening and detection of diseases that have PROVEN and well-established, life-saving treatments then our system is broken.
Our matrices and models are missing critical data elements and considerations. The #patientexperience. The health economic considerations of the individuals and families LIVING with the conditions. The expert providers who care for the patients who are detected too late for optimal interventions. Real data about harm of delayed diagnosis vs harm of false positive. Patient community members as VOTING members on the ACHDNC. And organizational representatives who are permitted to speak during critical discussions — and VOTE during life and death matters.
The lived experience of the #rarediease community MUST become required data consideration.
Thank you to the AC members who tried to make it so today.
Thank you to the Krabbe community for your evidence-based and impactful engagement today.
We have MUCH work to do to ensure that our newborn screening system is truly an equitable public health system.
And this is what Dylan Simon from EveryLife said during the Public Comment time the following day:
Highlights of #EveryLife‘s testimony to the federal #newbornscreening Committee this morning as drafted by Annie Kennedy and Dylan Simon in collaboration with #raredisease colleagues (amended due to LinkedIn character limits):
Dear ACHDNC:
Yesterday’s discussion and vote yielded a vote of 7-7. That tie vote was interpreted at the conclusion of the Committee meeting as a vote to NOT move Krabbe disease forward for consideration to the RUSP by the Secretary. The rare disease community urges this Committee to reconsider the interpretation of the tie vote. Indeed, yesterday did not yield a ‘no’. Instead, it yielded a need for further clarification of questions that were raised during the discussion that could not be addressed by participating members of the discussion.
The AC Charter Title XI § 1111 (42 U.S.C. § 300b-10) Section C Membership Item 1 states that – “… the Secretary shall ensure that the total membership of the Advisory Committee is an odd number.” While the Charter does not explicitly require that the purpose of the composition of membership being an odd number is to ensure that no vote ever end in a tie, we believe strongly that providing a path forward for further discussion and resolution of this tie is in keeping with the intention with which this Committee was established. We urge the Committee to revisit the conclusion of yesterday’s vote and consider options to ensure that the Krabbe disease nomination receives the full and complete consideration that it is deserving.
Related to the composition of the members of the Committee:
· We – once again – request the Committee add a patient representative as a voting committee member. Discussions that articulate and project experiences and opinions onto a community that lacks formal representation reflect a significant imbalance in representation.
· During every discussion of an evidence review, we ask the Committee formally include an expert member of the nominated disease community to participate in the discussion to be available to address questions that arise and inform the discussion.
o As examples, yesterday’s Committee discussion included significant time devoted to concerns around the impact screening might have on families identified as false positives based on older literature and practices that have since been updated.
o Yesterday’s discussion also included discussion of late onset phenotypes of the condition when the nomination was specific to infantile-onset Krabbe.
· During the conduction of the evidence review discussion, we urge that Organizational Representatives be permitted to participate in the discussion. As they have been invited on to the Committee because of the fact that they represent stakeholder groups who are vital within the newborn screening ecosystem, silencing their perspectives at the time they arguably matter most negates the purpose of their membership.
· Yesterday’s discussion contained thorough discussion about the perceived negative impact of receiving a late-onset diagnosis for families. However, recent data from the Babyseq experiment showed that at three months following their participation, 86.8 percent of parents were very interested in receiving information on their baby’s risk of developing a disease in childhood that can be prevented, treated, or cured. In addition, 84.6 percent were interested in receiving information regarding the on their baby’s risk of developing a disease in adulthood that could be prevented, treated, or cured.
The outpouring of support from the Rare Disease community has been healing for my heart. I saw comment after comment from various advocacy groups willing to help us in whatever we decide to do next because this could impact their condition when it’s their turn, too. The actions of the ACHDNC last week were unjust and must be made right.
The Krabbe advocacy community is developing a plan and we will be acting as quickly. What happened to the Krabbe Disease community on Thursday was not right, and yes, I am fully biased but that doesn’t blind me to injustices and inaccuracies. I know the science, I’ve seen the data, and I believe the doctors who have spent decades working toward this nomination more than I believe a committee of non-experts.
- I am a parent who heard the phrase “there’s nothing we can do” on Diagnosis Day, eight years ago yesterday.
- I am a parent who learned in that same conversation that had Tori been screened for Krabbe Disease at birth they could have treated it.
- It is the PARENTS’ choice whether or not to pursue treatment. It’s their risk to assume. But, without Newborn Screening, they are robbed of that choice and left with despair over what could have been.
A couple more things to add:
- The two most recent conditions that were added to the RUSP had lower grades than Krabbe was given
- One of the committee members published a paper in 2013 against screening for Krabbe Disease and I believe she should not have been allowed to vote (spoiler alert: she voted no) though I had hoped she would have changed her mind given the tremendous advances that have happened in ten years.
- A disease expert should have been involved in the final discussion to clear up any misconceptions. Some “opinions” are worth more than others.
I was asked yesterday what we do now and my honest answer is that I’m uncertain. I know that whatever the Krabbe community comes up with will be powerful and I will do my part to see us get the appeal we – and the babies in FORTY STATES – deserve.
I will leave you with words from Christin Webb – a mother and advocate who lost a daughter to Krabbe Disease and has a son who received a stem-cell transplant. I think her words capture it all.





Leave a comment